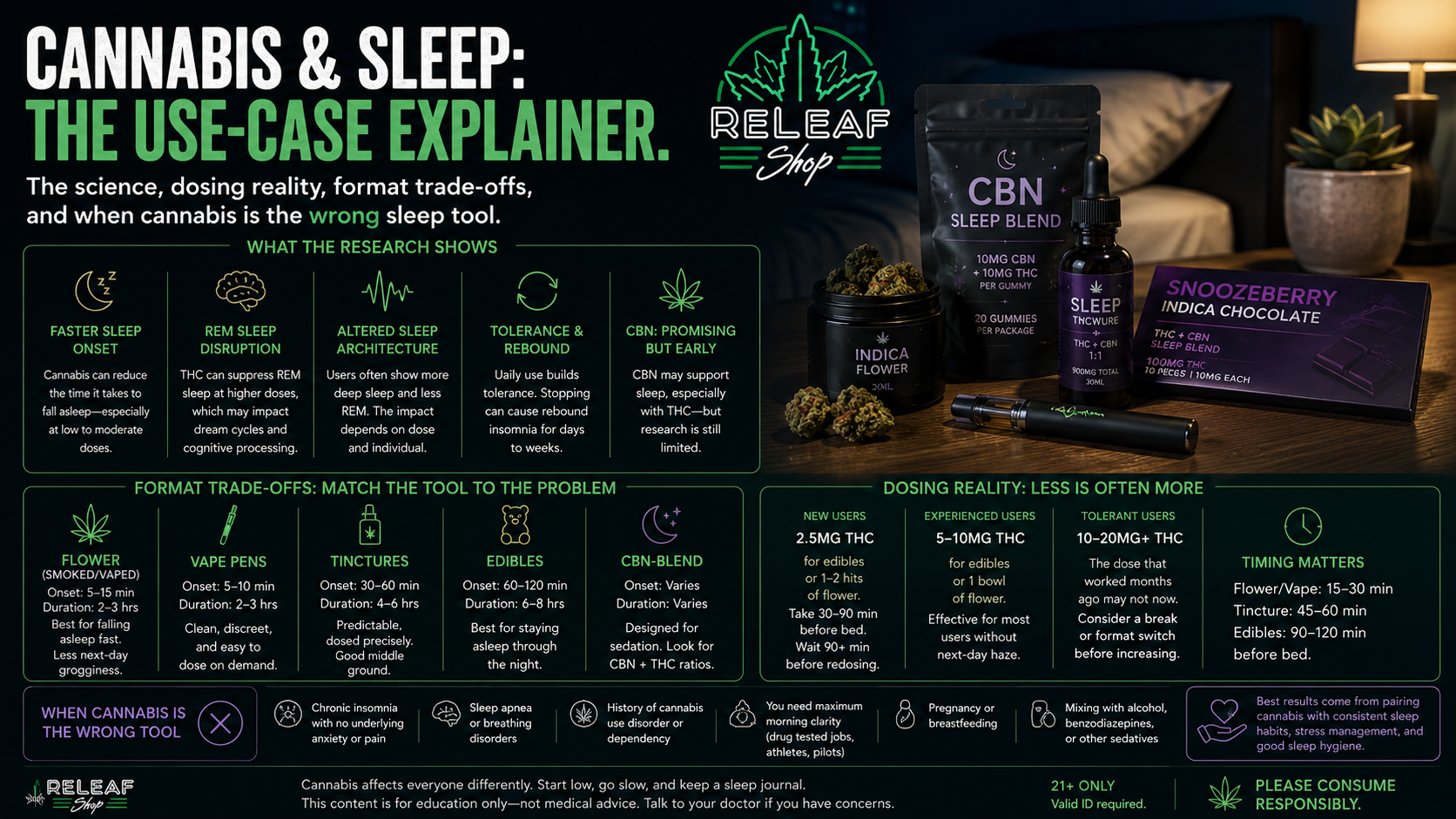
Use-case explainer rather than strain list. The science, dosing reality, format trade-offs, and when cannabis is the wrong sleep tool.

Cannabis can help you fall asleep faster. It can also disrupt your sleep architecture in ways you won't notice until you stop using it. Both are well-documented in the research, and the practical question for someone considering cannabis as a sleep aid isn't "does it work" but "under what conditions, with what trade-offs, and at what point does it stop being the right tool."
This guide is the use-case explainer for cannabis as a sleep aid — the science, the realistic effects, and the cases where cannabis isn't the right tool. Strain-specific recommendations rotate by batch; ask the budtender for current sleep-leaning options when you visit.
The research picture on cannabis and sleep is more nuanced than the marketing suggests.
Sleep onset. Multiple studies show cannabis can reduce the time it takes to fall asleep, particularly in users who experience sleep onset difficulty due to anxiety, racing thoughts, or physical tension. The effect is most pronounced at low-to-moderate THC doses; higher doses can produce paradoxical activation in some users.
REM sleep disruption. THC suppresses REM sleep at higher doses. Users who consume nightly often experience reduced dream recall and altered REM patterns. The clinical significance of this varies — some research suggests it benefits PTSD patients with traumatic dreams; other research raises concerns about cognitive consolidation that depends on REM sleep.
Sleep architecture changes. Cannabis users often show altered sleep stage distribution — more slow-wave sleep, less REM. Whether this is net beneficial or net harmful depends on the user, the dose, and the underlying sleep issue.
Tolerance and rebound. Daily cannabis use builds tolerance to the sleep-aiding effects within weeks for most users. Stopping after sustained use often produces rebound insomnia and disrupted sleep for days to weeks.
CBN research. CBN (cannabinol) is marketed for sleep based on early research suggesting sedating effects, particularly in combination with THC. The evidence is preliminary; clinical trials are limited.
The honest summary: cannabis affects sleep in real and complex ways. It's not a clean sleep aid; it's a tool with trade-offs.
Brief because the strain-specific picks rotate frequently. The framework below is what's durable.
Indica genetics. The indica/sativa label is rough but useful as a starting filter. Indica-dominant strains generally lean sleepier than sativa-dominant strains. Within a given strain, batch-level variation can matter as much as the genetic label.
Myrcene. The most common sleep-associated terpene. Found in heavy indica strains, mango, and hops. Strains high in myrcene tend to read sedating.
CBN. A minor cannabinoid associated with sedation. CBN-blended products combine THC and CBN in specific ratios marketed for sleep. The Snoozeberry indica bar from Incredibles is a recognizable example.
Linalool and beta-caryophyllene. Secondary terpenes associated with relaxation rather than direct sedation. Useful for users whose sleep issues are anxiety-driven rather than physical-tension-driven.
Format choice matters as much as strain choice for sleep-specific outcomes.
Flower (smoked or vaporized). Onset 5–15 minutes. Duration 2–3 hours. Best for users who want fast sleep onset without lingering effects in the morning. The short duration means cannabis is metabolized out of the system before the next day, reducing morning grogginess risk.
Edibles. Onset 60–120 minutes. Duration 6–8 hours. Best for users who wake up frequently during the night — the long duration covers the full sleep cycle. Worse for users sensitive to morning grogginess; the long duration sometimes lingers into the next day.
Tinctures. Onset 30–60 minutes. Duration 4–6 hours. Middle path between flower and edibles. Useful if you want predictable timing and dose control without the fast-onset nature of inhaled cannabis.
CBN-blend products. Available across formats — chocolate bars, gummies, tinctures, occasional flower. The CBN content claims specific sleep-leaning effects beyond what THC alone produces.
Vape pens. Onset 5–10 minutes. Duration 2–3 hours. Similar profile to flower with cleaner dose precision. Discreet and useful for users who want to avoid smoke smell.
The format-to-sleep-issue match is the practical decision point. Trouble falling asleep? Fast-onset format (flower, vape, sublingual tincture). Waking up at 3 AM? Long-duration format (edibles or oral tincture).
The most-skipped piece of cannabis-and-sleep advice: smaller doses generally produce better sleep outcomes than larger doses.
Cannabis has a steep dose-response curve. A small amount (5–10mg of THC, or 1–2 hits of flower) often helps with sleep onset without lingering grogginess. A larger amount (20mg+ THC, or a full bowl of flower) often produces sedation followed by morning haze and disrupted next-day functioning.
For new users. Start at 2.5mg of THC for edibles or one to two hits of flower. Take cannabis 30–90 minutes before bedtime depending on format. Don't redose during the wait period for edibles — the slow onset makes redosing the most common dosing mistake.
For experienced users without sleep tolerance. 5–10mg of THC for edibles, or one bowl of flower. Sleep effects without significant morning impact for most users in this dose range.
For tolerant users. The dose that produced sleep effects six months ago may not now. The fix isn't always more cannabis — it might be a tolerance break or a format switch.
Time it correctly. Take edibles 90–120 minutes before bedtime. Smoke or vape 15–30 minutes before. Tincture 45–60 minutes before. The wrong timing is one of the more common reasons cannabis-as-sleep-aid doesn't work — you peak at midnight when you needed to peak at 11 PM.
Our guide to how THC interacts with the body covers the absorption and clearance science in more depth.
Worth naming directly. Cannabis isn't the right answer for every sleep problem.
Sleep apnea. Cannabis can suppress upper-airway muscle tone, potentially worsening obstructive sleep apnea. Users with diagnosed or suspected sleep apnea should talk to a sleep clinician before using cannabis as a sleep aid. The trade-off can be net negative.
Heavy daily use. Cannabis use disorder is real, and one of its first signs is sleep dysfunction when use stops. If you've been using nightly for months and can't sleep without it, that's a sign to talk to a clinician about a tolerance break or treatment plan rather than escalating doses.
REM-dependent recovery. Cannabis suppresses REM sleep at higher doses. For users recovering from physical or cognitive demands that depend on REM sleep — athletes, students in heavy learning contexts, people processing trauma — sustained nightly use may interfere with recovery.
Severe insomnia. If you've gone weeks without adequate sleep, cannabis is unlikely to be a complete solution. Underlying causes — anxiety, depression, hormonal shifts, medication side effects, undiagnosed sleep disorders — deserve clinical attention. Cannabis may help on the margins; it doesn't replace evaluation.
Drug-test contexts. Cannabis is detected on standard drug tests for weeks after use. If your work or athletic context tests for cannabis, the conversation about sleep aids should happen with your clinician, not at a dispensary counter.
Pregnancy and breastfeeding. Cannabis is generally not recommended during pregnancy or breastfeeding regardless of the sleep question. Talk to a clinician about alternative approaches.
Our beginner's medical guide covers the broader question of when cannabis fits a treatment approach.
The often-skipped reality: stopping cannabis after sustained use commonly produces sleep disruption.
The rebound pattern. Users who consume cannabis nightly for weeks or months often experience days to weeks of rebound insomnia after stopping. Difficulty falling asleep, frequent waking, intense or unpleasant dreams as REM rebounds. This typically peaks in the first week and improves over 2–4 weeks.
Why this matters. The rebound period is the time when many users decide cannabis was "working" and resume use. The honest reality: cannabis was masking a sleep issue rather than treating it, and the rebound is what was always there underneath.
Practical approach. If you're considering stopping, plan for 2–4 weeks of disrupted sleep before assuming you've established a new baseline. Use the rebound period for clinical sleep evaluation if the underlying issue is severe.
Tolerance breaks. Periodic tolerance breaks (1–2 weeks off cannabis) can reset the dose-response curve and improve cannabis's sleep-aiding effect when use resumes. Some users build tolerance breaks into a regular cycle rather than treating them as cessation attempts.
Tapering vs. stopping. Some users find gradual dose reduction (over 2–4 weeks) more manageable than abrupt cessation. The research on tapering is limited but some clinical sleep specialists recommend it for established daily users.
Worth framing cannabis as part of a broader sleep approach rather than a single solution.
Sleep hygiene basics. Consistent bedtime, dark room, cool temperature, no screens for 30–60 minutes before bed. Cannabis works better when it complements these basics rather than replacing them.
Caffeine timing. Cannabis-as-sleep-aid is undermined by afternoon caffeine. The half-life is long; coffee at 2 PM still affects sleep at 11 PM for many users.
Exercise and natural light. Both improve sleep architecture independently. Cannabis users who incorporate regular exercise and morning light exposure typically need lower cannabis doses for the same sleep outcome.
Anxiety and stress. If your sleep issue is anxiety-driven, addressing the underlying anxiety (therapy, meditation, lifestyle) typically produces better long-term outcomes than cannabis.
Clinical evaluation. Persistent sleep issues deserve clinical attention. A sleep clinician can identify underlying issues (sleep apnea, restless legs, circadian rhythm disorders) that cannabis won't fix and may mask.
Cannabis can help some people fall asleep faster, especially when sleep difficulty is linked to anxiety, racing thoughts, or physical tension. But it is not a perfect sleep aid, and the trade-offs can include REM sleep disruption, tolerance, and rebound insomnia after stopping.
It depends on the use case. THC is more commonly associated with helping users fall asleep faster, while CBD may be more useful when sleep problems are tied to anxiety. Many users find balanced THC/CBD products helpful, but the right fit depends on the person and the underlying sleep issue.
Yes. Higher-THC cannabis use can suppress REM sleep, which often reduces dream recall and changes sleep architecture. That may be useful in some cases, such as trauma-related dream disturbance, but it can also create trade-offs in long-term sleep quality and recovery.
Sometimes. High THC doses can paradoxically feel activating for some users, and daily use can lead to tolerance, meaning cannabis becomes less effective over time. When regular users stop, rebound insomnia is common and may last days to weeks.
The best format depends on the sleep problem. Flower and vape pens work best for people who mainly struggle to fall asleep because they act quickly. Edibles and oral tinctures are usually better for people who wake up in the middle of the night because they last much longer.
Flower is usually better if you want fast onset and less risk of next-morning grogginess. Edibles are often better if you need longer-lasting effects to stay asleep through the night. The trade-off is that edibles take longer to kick in and are more likely to linger into the next day.
For new users, the article recommends starting low: about 2.5mg THC for edibles or one to two hits of flower. The key is to give it enough time to work before taking more, especially with edibles.
Timing depends on the format. Edibles generally need 90–120 minutes before bedtime, tinctures around 45–60 minutes, and flower or vape pens about 15–30 minutes. Bad timing is one of the main reasons cannabis does not work well as a sleep tool.
It can. Morning grogginess is more likely with higher THC doses and longer-lasting formats like edibles. Lower doses and faster-clearing formats such as flower or vape pens usually reduce that risk.
CBN is commonly marketed for sleep, and some early research suggests it may have mild sedating effects, especially when combined with THC. But the article makes clear that the evidence is still preliminary and not as strong as many marketing claims suggest.
Myrcene is the terpene most commonly associated with sedating, sleep-leaning effects. The article also notes linalool and beta-caryophyllene as useful supporting terpenes, especially when the sleep issue is more anxiety-related than purely physical.
Nightly use deserves caution. Regular use often builds tolerance within weeks, can alter REM sleep over time, and may create dependence on cannabis for sleep. The article frames cannabis as a tool with trade-offs, not a clean long-term sleep solution.
Cannabis may be the wrong choice for people with sleep apnea, severe chronic insomnia that needs medical evaluation, pregnancy or breastfeeding, drug-testing obligations, or signs of cannabis dependence. The article also notes that persistent sleep problems often deserve clinical attention rather than just escalating cannabis use.
After sustained nightly use, many people experience rebound insomnia, more frequent waking, and vivid or unpleasant dreams as REM sleep rebounds. This usually peaks in the first week and often improves over two to four weeks.
Cannabis can help with both, but different formats fit different needs. Fast-onset formats like flower and vape pens are usually better for falling asleep, while longer-duration formats like edibles and oral tinctures are better for staying asleep through the night.
Cannabis can help with sleep when used thoughtfully — the right dose, the right format, the right timing, in combination with sleep hygiene basics rather than as a standalone solution. It's not a clean sleep aid; it's a tool with trade-offs that vary by user. For occasional sleep difficulty, low-dose cannabis is one reasonable approach. For chronic sleep issues, the cannabis question deserves a clinical conversation alongside the dispensary one. The live ReLeaf menu shows what sleep-leaning options are currently in stock; the overview of THC product types covers format options.




